A medical error is a preventable adverse effect of care, whether or not it is evident or harmful to the patient. This might include an inaccurate or incomplete diagnosis or treatment of a disease, injury, syndrome, behavior, infection, or other ailment.
This is Wiki's definition of a medical error.
Can I just say that I NEVER want to be responsible for a medical error that causes someone harm or worse yet, death!
We researched and reviewed errors this week for our Safety class. We read the story of a young mother who died as a result of care she received at a hospital. There are actually many stories like this and I think it is important that these stories get heard.

Every time I read a story about an error in patient care that resulted in injury or death I am reminded of how important what I do and don't do are. As much as it is hard to read these stories it is so essential that they are in the forefront of my mind because I need to be ever vigilant in all my actions and procedures so I do not cause harm. I didn't get into nursing to hurt, I became a nurse so I could help.

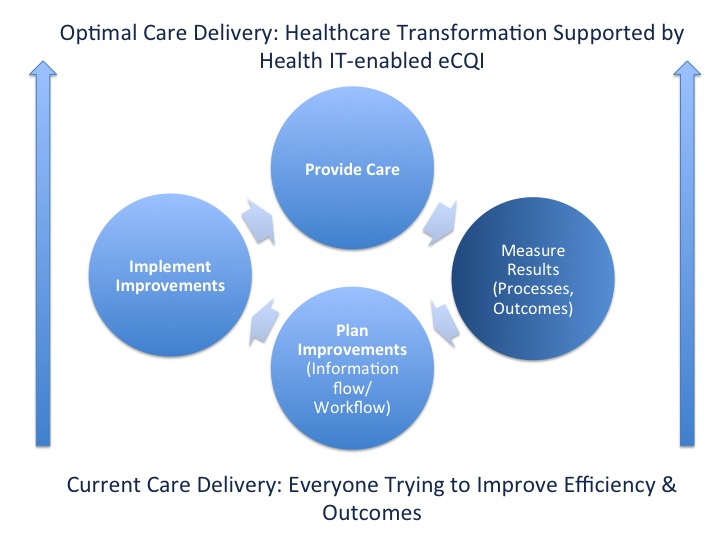
Many errors that have occurred have resulted in a change in policy or procedure for patient care. These areas include trauma care, anesthesia monitoring, fetal heart monitoring, wrong site amputation or surgery, sponge counts, fatal allergies, potassium mishaps, decubitus ulcers, and lifting techniques. It is unfortunate that some patients and families suffered, but at least their suffering led to saving the lives of others.
As nurses and professionals we have policies and procedures in place to protect our patients and ourselves from the adverse reactions of errors.... Follow them!!! Use the six rights of medication administration (right patient, right med, right time, right route, right dose, right documentation). There are things we can do to make sure we don't cause harm.

Even though I am new at nursing, here are some of my suggestions:
Slow down
Don't take any procedure or process for granted
If it doesn't seem right, feel right, look right.....ask for help!
When in doubt, look it up or ask your charge nurse
Listen to the patient and their family
Always assess
Take a step back and review
Always double check when it is required (and sometimes if it isn't)
There are many ways we can support our industry and provide patient-centered safe care. They are all available to us, but it is up to us to utilize what we know and reach out when help is needed. Safety saves lives and those lives are in our hands!